With the extensive outbreak of Covid-19, the government and public health department brought in mandatory lockdown of the entire country with social distancing, quarantine and isolation of millions. These measures definitely had an impact in halting the progress of the virus in the community. But in the post-lockdown period, the case load is predicted to rise as the movement of people increases bringing along with it extensive socio-economic and political crisis.
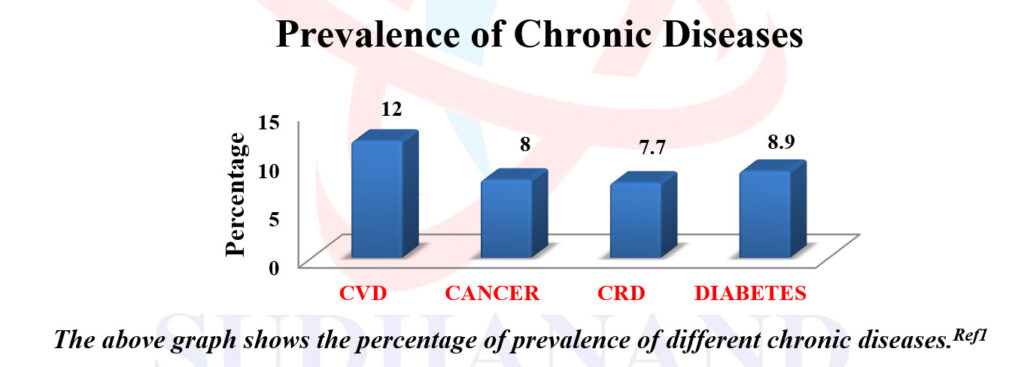
As a result of this there is a need to keep the patients with co-morbid conditions who are at a higher risk of getting severely affected by Covid-19 away from the general population. This is corroborated by several studies conducted all over the world. In one such study the risk of developing severe disease in patients with hypertension was 13.0-27.2%, diabetes 7.2-12.2%, followed by cardiovascular disease 3.8-13.8% and respiratory system disease 0.9-2.1% Ref: 1.
The current world statistics according to the WHO indicates that the case load of Covid-19 stands at a staggering 16,80,40,871. The total number of deaths due to Covid-19 is 34,94,758. In India, there are currently 2,73,69,093 active Covid-19 cases and 3,15,235 deaths as on 27 th May, 2021. A substantial number of these deaths are of people belonging to age group of >60 years, most of them with co-morbidities.
Adding to this burden are the asymptomatic carriers of the disease who are a potential infection source of Covid-19 Ref 2. Therefore modifications in public health measures, health systems and community preparedness would be critical in mitigating the spread of Covid-19 in the country.
Bearing this in mind, we at Dr. M. D. Sachidananda Murthy Memorial Trust in association with SAS Poorna Arogya Health Care and Dr. M. D. Sachidananda Murthy Memorial Group of Hospitals came up with an idea of a vehicle – “Sudhanand Arogya Vahini”, which could go door-to-door and conduct various laboratory tests pertaining to their existing conditions as well as provide a means of getting them in touch via Telemedicine with a doctor who could give them sound medical advice, thereby preventing them from coming in contact with potential source of infection.
This method also serves a dual purpose. It will be used to collect data regarding age, sex, travel history, existing symptoms and pre-existing co-morbid conditions. There is a possibility of detecting previously undiagnosed diseases as well.
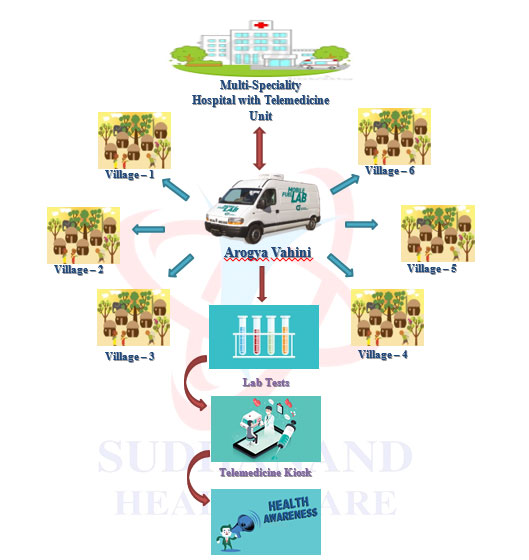
SAV will be equipped with a Haematology Analyzer, Biochemical Analyzer, ECG Machine, Sphygmomanometer and Pulse Oximeter. It will consist of a sink, soap dispenser, cupboards, waste bins, chairs along with having power and water supply. One of the main components of this vehicle is a “Tele-Communication Kiosk”, which consists of a computer that will form a doctor-patient interface and a printer which will be used to deliver reports of laboratory tests to the patients. Lab reports will also be delivered to patients’ registered mobile numbers in view of maintaining confidentiality and conserve paper.








The vehicle will be manned by a trained nurse, lab technician and a driver. The nurse will collect details of the patient and log it. She will determine the symptoms and will be able to prescribe relevant tests for which the lab technician shall collect the appropriate samples and run the tests. For example, if a patient is diabetic with kidney problems, then the nurse will prescribe a blood sugar analysis (FBS/PPBS/RBS/HbA1c) and renal function tests (blood urea, serum creatinine, uric acid). An ECG shall be done if there is a history of cardiac disease.
Since the nurse will be trained, she will be able to diagnose/order appropriate tests for people who have no history of pre-existing disease but have symptoms. This data will help in detecting new cases in the population at an early stage thereby halting the severity of diseases which could otherwise become life threatening in the current scenario.
These are an array of investigations that can be done at the SAV at subsidized costs. Reports of lab investigations shall be given to the patient for future use.
The idea of a Tele Communication Kiosk was perceived bearing in mind the psyche of the population, as people are more satisfied after discussing their symptoms/disease with a doctor. The lab reports of patients whose samples are collected will be relayed in real time to a doctor situated at Dr. M. D. Sachidananda Murthy Memorial Hospitals and will be reviewed by him/her. Further advice regarding any other tests to be conducted or a treatment protocol to be followed will be advised to the patient via the communication desk. A report of the investigations that were carried out will be provided to the patient at the door step for future reference. The main impact is that the kiosk will prevent patients from coming to the hospitals, thereby preventing exposure to a potential source of infection.
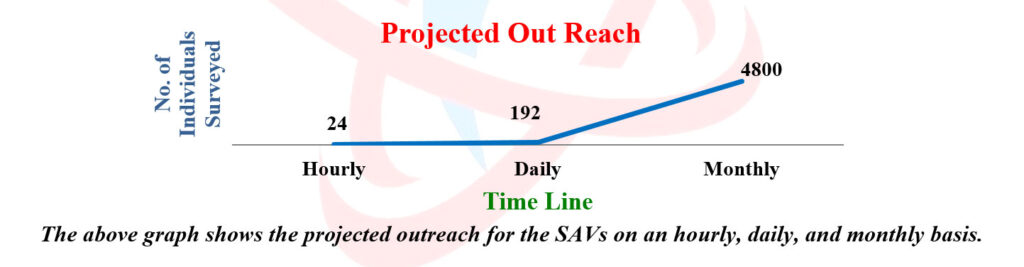
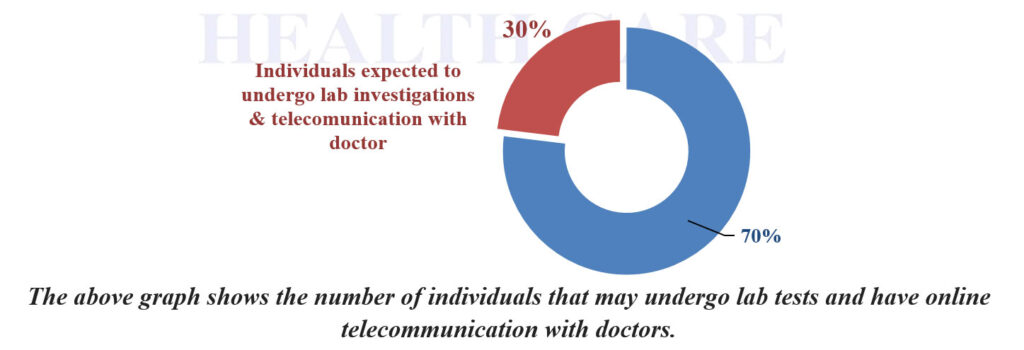
The staff at SAV is expected to work about 8 hours a day from 8am to 5pm with one hour of break time. We expect to cover 6 houses/families an hour which would account to surveying 48 houses a day, 1,200 a month. With an average of 4 people per family, we aim to reach up to 4,800 individuals a month.
Among these people, about 30% would be expected to undergo lab investigations and Tele-Communication with a doctor, which will be done for about 1,440 people in a month, as seen below.
An extensive demographic survey was done and a 50-80 km radius around the 4 hospitals was earmarked for collecting data and running this program. Accordingly, the number of villages around Disha Hospital (Mysore), Dharani Hospital (Chamarajanagar), Kaveri Hospital (Kushalnagar) and Krishna Hospital (Bettadapura) are approximately 123, 179, 291, and 196 respectively. We aim to survey and cater to 19,200 of the population in a month through SAV.
R0 which represents the number of new infections that might stem from a single case is around 1.5-1.6 in India currently. So keeping in mind that this program covers 19,200 of people per month and applying the current R0 to it, even if 1% of this population is infected, they can potentially spread the disease to 307 people.
Also, 8.5% of Indian population is geriatric (According to 2016 report from Ministry of Statistics) and is at a higher risk of developing the disease and the risk only increases if they come into contact with asymptomatic carriers of the disease.
Through this program, we aim
Ref1 – Prevalence of comorbidities and its effects in coronavirus disease 2019 patients: A systematic review and meta-analysis. Yang J et al. Int J Infect Dis. 2020 Mar 12;94:91-95. doi: 10.1016/j.ijid.2020.03.017.
Ref2 – Delivery of infection from asymptomatic carriers of COVID-19 in a familial cluster, Feng Ye.International’s journal of infectious diseases.